







The World Obesity Federation predicts that by 2030, approximately one billion people will be living with obesity worldwide, and this represents that 1 in every 5 women and 1 in every 7 men will be obese. The prevalence of obesity is set to double between 2010 to 2030 in Southeast Asia [1]. In Malaysia alone, 1 in 2 Malaysians are considered overweight or obese. In view of alarming obesity rates and evolving evidence in obesity management, Malaysia has just released a 2023 Clinical Practice Guideline (CPG) update on the management of obesity, after almost two decades [2]. This CPG aims to help healthcare professionals at all levels understand the importance of weight management and to assess and manage their patients effectively. The full guideline can be accessed here.
Screening and diagnosis of obesity
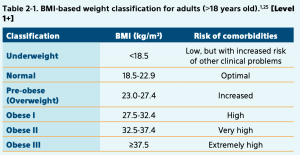
It is recommended that all adults should have their body mass index (BMI) assessed annually, and those with a BMI of ≥ 23 kg/m2 should be further evaluated.
Asians have a lower BMI cut-off point for overweight and obesity compared to Caucasians, due to evidence from Asian countries showing that the risk of comorbidities such as type 2 diabetes mellitus (T2DM), hypertension and other cardiovascular diseases begin to increase at lower BMI.

Waist circumference (WC) is a convenient method to assess excess fat around the abdomen – high abdominal or visceral fat is an independent risk factor for cardiovascular disease (CVD).
In Asians, a WC of >90cm for men and > 80cm for women indicated a higher risk of T2DM and CVD.
Patients who are pre-obese and above should be assessed for the following conditions and current medication history should be elicited to evaluate if weight gain is due to medication side effects.
- Hypertension
- T2DM and Prediabetes
- Metabolic syndrome
- Dyslipidaemia
- Obstructive Sleep Apnoea (OSA)
- Osteoarthritis/Degenerative joints/back pain
- Metabolic Associated Fatty Liver Disease (MAFLD)
- Gastroesophageal Reflux Disease
- Cancer
Treatment goals
The main treatment goals in obesity management are to
- Prevent metabolic complications and manage existing comorbidities
- Fight stigmatization against obesity and restore individual’s well-being and self-esteem
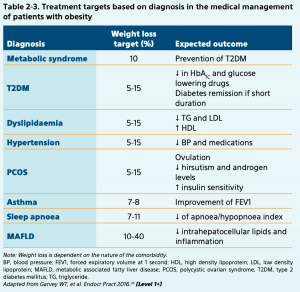
Weight loss goals should be tailored according to the patient’s complications, as summarized below:

Lifestyle modifications in the management of obesity
Managing overweight and obesity includes a combination of dietary modifications and increased physical activity. Physicians should work together with a dietician to come up with an individualized dietary plan based on age, sex, readiness level, physical activity level, comorbidities and patient preference. In general, there should be a restriction of 1200-1500 kcal/day and 1500-1800 kcal/day for women and men respectively. Alternatively, to reduce 500-750 kcal from baseline intake.
Physical activity and exercise can also significantly reduce weight and improve health when combined with caloric restriction. Patients should engage in a minimum of 150 min/week progressing to 300 min/week of moderate-intensity exercise or 75-150 min/week of vigorous-intensity exercise. As a guide, moderate-intensity exercise allows for talking and not singing while vigorous-intensity exercise does not allow for talking or singing.

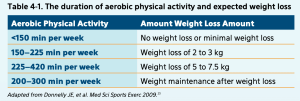
Lifestyle modifications should be enlisted to help patients achieve the following weight loss goals:
- Up to 1 kg per week
- Up to 10% of baseline body weight
- A total of 3-5% of baseline body weight in the presence of cardiovascular (CV) risk factors (e.g., hypertension, hyperlipidaemia and hyperglycaemia)
Pharmacotherapy in the management of obesity
Pharmacotherapy should be considered when weight loss or weight maintenance cannot be achieved with lifestyle interventions alone. Patient populations indicated for pharmacological treatment include:
- BMI 27 – 29.9kg/m2 with concomitant T2DM, hypertension, dyslipidemia or obstructive sleep apnoea (OSA)
- BMI >= 30kg/m2 with or without the above concomitant conditions
Drugs indicated for obesity
| Orlistat | Phentermine/
Topiratmate |
Naltrexone/
Buproprion |
Liraglutide | Semaglutide | |
| Route | Oral | Oral | Oral | Subcutaneous injection | Subcutaneous injection |
| Mean weight loss in excess of placebo | 2.6kg | 8.8kg | 4.95kg | 5.24kg | 12.7kg |
| Common side effects | Abdominal cramps
Oily stools Flatulence with discharge Reduced absorption of fat soluble vitamins A,D,E,K |
Dry mouth
Insomnia Constipation Paresthesia |
Nausea | Nausea, vomiting, diarrhea, constipation | Nausea, vomiting, diarrhea, constipation |
| Additional benefits | Reduces glucose levels
Reduce insulin resistance Reduce lipid levels |
Reduction in HbA1c
Reduce insulin resistance Reduces lipid levels Reduces BP |
Reduction of HbA1c
Reduces BP Reduces lipid levels |
Table 4: Recommended drugs for obesity
Surgical procedures
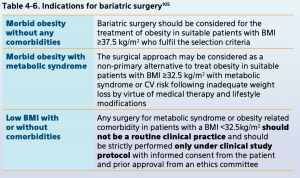
Bariatric surgery is indicated when severely obese individuals are unable to achieve weight loss after 6 months of lifestyle modification and pharmacotherapy.

There are 3 types of procedures, namely Roux-En-Y gastric bypass (RYGB), Sleeve gastrectomy (SG) and Abdominal gastric binding (AGB)
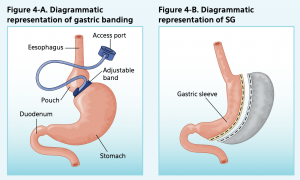
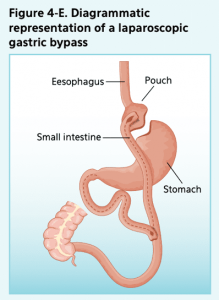


From the left, Figure 1: Diagrammatic representation of gastric banding (AGB), sleeve gastrectomy (SG) and laparoscopic Roux-En-Y gastric bypass (RYGB)
RYGB produces the largest percentage weight loss at 1 year at 31.2%, followed by 25.2% for SG and 13.7% for AGB. However, RYGB does have a longer list of possible postoperative complications compared to the other 2 bariatric procedures.
Conclusion
Management of obesity requires the combined effort of a multidisciplinary healthcare team. In addition, more awareness needs to be raised on obesity as a chronic disease and individuals in the society should be educated on lifestyle modifications to prevent obesity, and to also seek professional help when required.
References:
- Tham KW, Abdul Ghani R, Cua SC, et al. Obesity in South and Southeast Asia-A new consensus on care and management. Obes Rev. 2023;24(2):e13520. doi:10.1111/obr.13520
- Clinical Practice Guidelines: Management of Obesity 2nd Edition 2023. Ministry of Health Malaysia








 for HIV Treatment")
